|
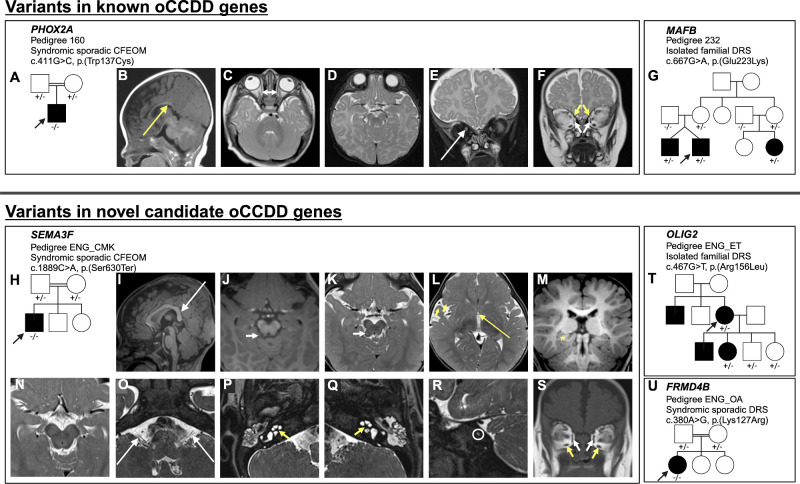
Figure 8.
The oCCDD pedigrees with functionally validated candidate genes/variants and brain MR images of probands with homozygous

|
|
Figure 8.
The oCCDD pedigrees with functionally validated candidate genes/variants and brain MR images of probands with homozygous