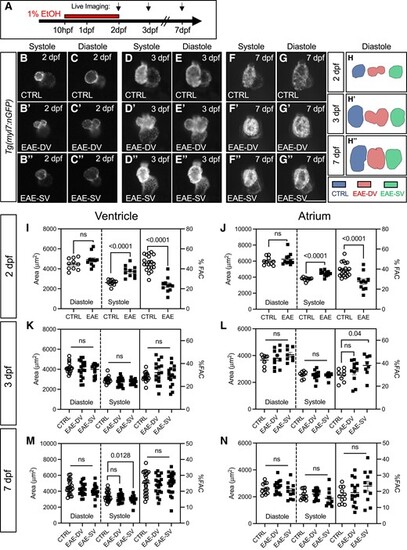
EAE causes persistent abnormalities in ventricular shape and acute recoverable systolic failure. A. Schematic of EtOH exposure windows. B–G’’. Live imaging of CTRL and EAE Tg(myl7:nGFP) hearts at 48, 75, and 168 hpf in systole and diastole. H–H’’. 2D traces of ventricular chamber shape in representative CTRL, EAE-SV, and EAE-DV samples at 48, 75, and 168 hpf. I–J. Quantification of ventricular (I) and atrial (J) chamber area and %FAC from live-imaged CTRL and EAE (EAE-SV and EAE-DV combined) Tg(myl7:nGFP) hearts (n > 10, 48 hpf). EAE hearts have evidence of acute systolic failure. K–L. Quantification of ventricular (K) and atrial (L) chamber area and FAC from live-imaged CTRL, EAE-DV, and EAE-SV Tg(myl7:nGFP) hearts (n > 8, 75 hpf). M–N. Quantification of ventricular (M) and atrial (N) chamber area and FAC in live-imaged CTRL, EAE-DV, and EAE-SV casper;Tg(myl7:nGFP) hearts (n > 11, 168 hpf). Data are presented as the standard error of the mean. Statistical significance was determined by an unpaired, two-tailed Student's t-test assuming equal variances (I–N). P-values are shown. Scale bars: 100 μm. ns, non-significant (P > 0.05).
|
